
{kind=link}
{kind=link}
{kind=link}
Understanding Jaw Joint Function and Derangement
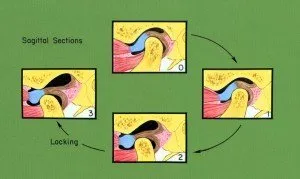
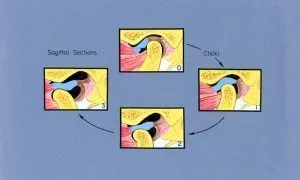
The signs of a jaw joint (TMJ) derangement are basic and quite simple. Pain when chewing, jaw popping, and locking of the joint such that the mouth will not open or the jaw gets stuck open or locks open are basic problems. They can create earache type pain and pain with all attempted jaw movement and function. A derangement in any joint is a mechanical problem between the moveable boney components and cartilage parts of the joint.
Movements of any joints by the muscles of the body have consequences. Whenever joints move, physical forces are distributed within cartilage and ligament structures that support that joint. Acute injuries will at least sprain joint ligaments and at worst tear or create bleeding within or around those ligaments or cartilage tissues. Tears create problems with joint function and rarely heal themselves completely.
Joints with large displacement movements create forces that are distributed through ligament and cartilage tissues and eventually to surfaces of bone. As long as those forces are within what the joint was structured to withstand, normal function occurs. However, forceful movements or movements which exceed what the joint can withstand acutely or chronically create a derangement. The ligament systems no longer support the joint properly and other internal structures become damaged.
The jaw joint and the shoulder joint are very similar when it comes to function and injury. We are all familiar with rotator cuff injuries or tears in the shoulder. The development of TM joint derangements can be similar to what happens in the shoulder.
Relative to one another, the jaw joint and shoulder have large magnitudes of physical movement. The shoulder rotates significantly when we raise our arms, lift something, or perform a throwing motion. The TMJ rotates and then slides or glides to maximum mouth opening.

 When long term derangements of a joint exists, abnormal movements may create changes to the bone surface structure between the ball (condyle), socket (fossa), and within the load bearing cartilage of the joint. The “cartilage” of the jaw joint is actually elastic connective tissue and has remarkable adaptive capabilities — but only up to a point.
When long term derangements of a joint exists, abnormal movements may create changes to the bone surface structure between the ball (condyle), socket (fossa), and within the load bearing cartilage of the joint. The “cartilage” of the jaw joint is actually elastic connective tissue and has remarkable adaptive capabilities — but only up to a point.
In the shoulder, a condition called an impingement often develops which is a narrowing of the joint space (critical separation between moveable boney components of a joint system) in critical regions of the joint. Tears in the rotator cuff occur when bone pressures damage the cartilage during function. Athletes who throw balls or other objects or perform other complex forceful joint movement can all be vulnerable to development of incomplete or complete tears of the rotator cuff from chronic forceful, repetitive motion.
With full mouth opening, forces within the TMJ are maximized. This joint is designed withstand tension or pulling forces which are created with both chewing function and mouth opening function. Tension forces over time influence changes in bone structure architecture in either the fossa (socket component) or condyle (ball component) which can create bone spur development which damages the functional cartilage component of the joint.
The most basic derangement of the TMJ can be a detachment or tear of the fibrous tissue capsule of the joint which then creates inflammatory pain and instability of the joint. Impingements of this joint system can develop and the consequence is very similar to what happens in the shoulder. Diagnosis is quite basic and includes an MRI examination in 3 dimensions.
Causes of Significant TMJ Disorders
Problems in the jaw joint that require surgery generally occur in young patients unlike the majority of patients who require surgeries for degenerative joint disease conditions of other joints of the body. This is because injured jaw joint cartilage can degenerate earlier and faster than other joints. The unique type of tissue and the gliding mechanics of the jaw joint system create destructive shear and torque forces when the disc/capsule of the joint is chronically unstable.
The jaw is vulnerable to trauma. Blows to the jaw and childhood falls and associated cuts to the chin area are common. Rarely is any concern expressed about pediatric jaw trauma. The child may receive stitches, perhaps an x-ray is taken to rule out a fracture, but joints are rarely imaged.
However, the amount of energy required to detach ligaments or rupture the jaw joint disc/capsule require 5-10% of the energy needed to break the jaw in the same area. Consequently, patients undergoing skeletal growth can have a true TM joint injury that may not be fully realized until years after the event when the joint can no longer glide appropriately and growth is complete. In older patients, blows to the jaw, hyperextension (sprain) injuries or any other event that could damage supportive ligaments can result in a derangement.
Infection in the jaw joint is another source of damage that can lead to severe TMJ disorders. Jaw joint infections are often overlooked and left untreated.
Finally, growth and development problems can lead to derangements of the jaw joint. The socket (fossa) of the joint develops as part of the base of the skull. The ball (condyle) develops along with lower jaw. Both have different developmental “programming”. Facial and jaw deformities can be associated with joint derangements. From an orthopedic perspective, if growth and development problems create a miss-match in the size or shape of boney parts of a gliding joint system, (ie. a condyle that is too large for the fossa component) a consequence can be damage to the cartilage disc/capsule during normal function.